



DARVO as Public Health Policy
How Politicians Blame Americans for Health Failures While Creating the Very Conditions That Make Health Impossible

Thank you to those who upgraded their subscriptions or made a one-time donation to Long Covid, MD! Your support bolsters my dedication to this field of medicine. If you haven’t upgraded yet, please consider.
There is no podcast episode this week. Instead, I’m sharing some thoughts on the political strategy I observe in public health discourse. These are my opinions on the systemic challenges to health in America, and the weaponization of chronic illness recently. Let me know how you’re viewing the situation. We’ll be back soon with another podcast episode.
DARVO as Public Health Policy
Earlier this week, I clicked on a video featuring FDA Commissioner Dr Martin Makary. Speaking to the camera, he said, “Today we’re talking about root causes of disease.” I expected to hear about preventive healthcare, access to nutritious food, the crushing cost of housing and childcare, and our underfunded public education system. Instead, the topic was talcum powder. I sighed and said to myself, “DARVO.”
DARVO is not a medical term, it’s a behavioral one most commonly used in popular psychology. The acronym stands for Deny, Attack, and Reverse Victim and Offender. Often used to describe abusive or narcissistic behavior, DARVO is a manipulative strategy that allows the guilty party to deny wrongdoing, go on the offensive, and blame the victim. It’s a tactic used to maintain control and avoid accountability. And tragically, it’s not just used in relationships. We’re now seeing DARVO on a national scale, where politicians and institutions blame Americans for poor health outcomes while simultaneously upholding systems that prevent healthy living.
DENIAL: Pretending the System Isn’t Broken
The most glaring example of denial? The declaration that COVID is over.
During a 60 Minutes interview in September 2022, President Joe Biden announced, "The pandemic is over…We still have a problem with COVID. We're still doing a lot of work on it. But the pandemic is over. If you notice, no one's wearing masks. Everybody seems to be in pretty good shape."
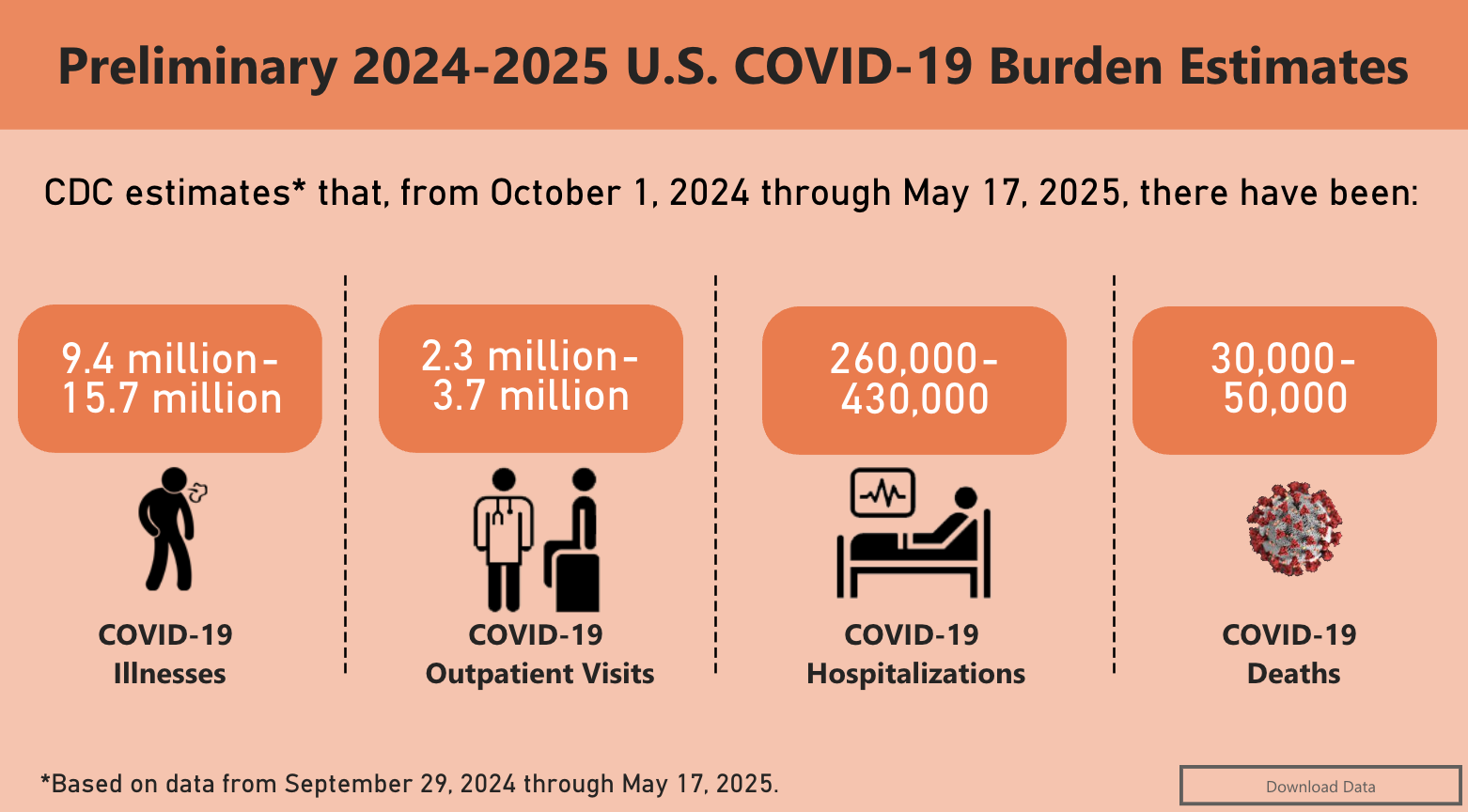
Of course, “no one’s wearing masks” is not a metric of public health. Millions of Americans continue to be infected with COVID each year. More than 40,000 people in the U.S. have died from COVID-19 in the past nine months alone. Even a mild infection carries the risk of long COVID, a chronic and debilitating condition that’s affecting millions.
In the absence of mask mandates, which were challenging to a society that deeply values personal choice, what was once a public health precaution has become politicized. Masking is variably enforced even in hospitals, and those who do choose to mask are often viewed as overreacting, or worse, as potential criminals. Some workplaces, like In-N-Out Burger, have gone so far as to ban employee mask use in certain states.
I will never forget White House press secretary Karine Jean-Pierre dismissing the suggestion that hospital masking policies might be a government concern, even during a period of extremely high viral spread of COVID-19, RSV and flu. “Look,” she sighed, “it’s up to each and every individual American to make the decision of what they want to do.”
If we’re expected to make “good choices” to stay healthy, travel, and remain employed for the good of the economy, how do we navigate a system that actively obstructs those choices?
ATTACK: Blaming Individuals for Systemic Failures
Dr. Mehmet Oz, now heading Medicare and Medicaid Services, recently argued that the U.S. isn’t getting a good return on its investment in these programs. He claimed that being healthy is an individual’s patriotic duty and said, “Seventy percent of what we spend on Medicare and Medicaid is on chronic illness, and we’re not getting our money’s worth.”
That’s not true.
The populations who qualify for Medicaid (based on age, disability, and income) tend to be in poorer health to begin with, and have higher rates of chronic disease. But research clearly shows that expanding Medicaid eligibility leads to better health outcomes, especially in preventive care. According to the Kaiser Family Foundation, adults with Medicaid outperform the uninsured on nearly every measure of preventive care.
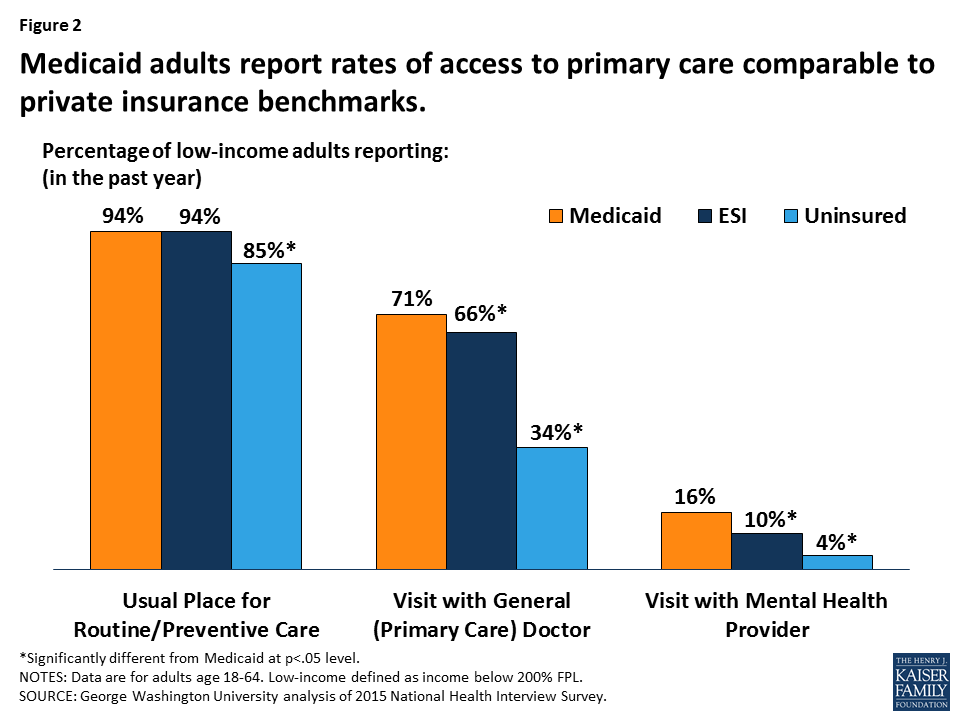
Increased access to Medicaid has been shown to raise screening rates for cancer, heart disease, diabetes, and depression, while reducing skipped medications and improving mental health outcomes. The data is unequivocal: Medicaid and Medicare are good investments. Yet time and time again, politicians denigrate and attempt to slash these programs.
Payments to physicians who care for Medicaid/Medicare patients - who tend to have more complex health issues - have been cut repeatedly, even as inflation and healthcare costs rise. Currently, new proposals threaten to gut the system even further, ignoring the simple truth: chronic diseases don’t vanish when you stop paying for treatment, and individuals cannot overcome their health burdens without adequate healthcare.
REVERSE VICTIM AND OFFENDER: Who’s Really at Fault?
Public health and political leaders have increasingly shifted the blame for poor health outcomes onto the people who need support the most. Americans are painted as the problem for needing help, while those in power who shape the policies that make staying healthy so difficult, rarely face accountability.
Recently, I heard House Speaker Mike Johnson discuss the cost of Medicare and Medicaid. “We have to eliminate [people] on Medicaid who are not actually eligible,” he said, “able-bodied workers, young men who should never be on the program at all.”
We’ll talk about the morality underpinning the phrase “young, able-bodied men” in a moment, because it connects to the recent FDA restrictions of the COVID-19 vaccine.
What’s Keeping Health Insurance Out of Reach?
First, let’s consider the systemic issues that Representative Johnson helps perpetuate keep many able-bodied young men's income low enough to be eligible for Medicaid.
Health insurance is linked to full-time employment that offer benefits. The alternative is paying steep premiums for private insurance.
Employers are not obligated to offer insurance benefits to part-time workers.
Low minimum wages make premiums inaccessible, even for those working multiple part-time jobs.
Higher education is expensive and increasingly out-of-reach, making it hard to follow flippant suggestions like “get a better job.”
Following the script of DARVO, American politicians like Johnson flip the roles of victim and offender. It is the sick and the poor person who is a drain on the government. Beneficiaries of public services are abusing the good nature of the people who have funded those services.
Victims are increasingly cast as the offenders - for needing help, for falling ill, for relying on social services - when the real offenders are the systems that create and perpetuate impossible conditions for health. These systems include government agencies, corporate employers, and public health leaders who withhold the very tools needed for well-being, then scold people for failing to thrive.
The New COVID Vaccine Policy: Withholding Protection
A prime example is the FDA’s new policy restricting COVID-19 vaccines to “high-risk” individuals, primarily those aged 65 and older. This decision effectively abandons younger people, even though we have abundant evidence that COVID can lead to long-term health issues in any age group. Chronic conditions like long COVID, cardiovascular damage, and immune dysfunction are not limited to the elderly.
Former Surgeon General Dr. Jerome Adams rightly criticized this policy, calling it an “age-based lottery” that leaves millions vulnerable. Instead of investing in widespread access to vaccines, we are repeating a pattern of reactive, short-sighted policy that blames individuals while stripping them of tools for protection.
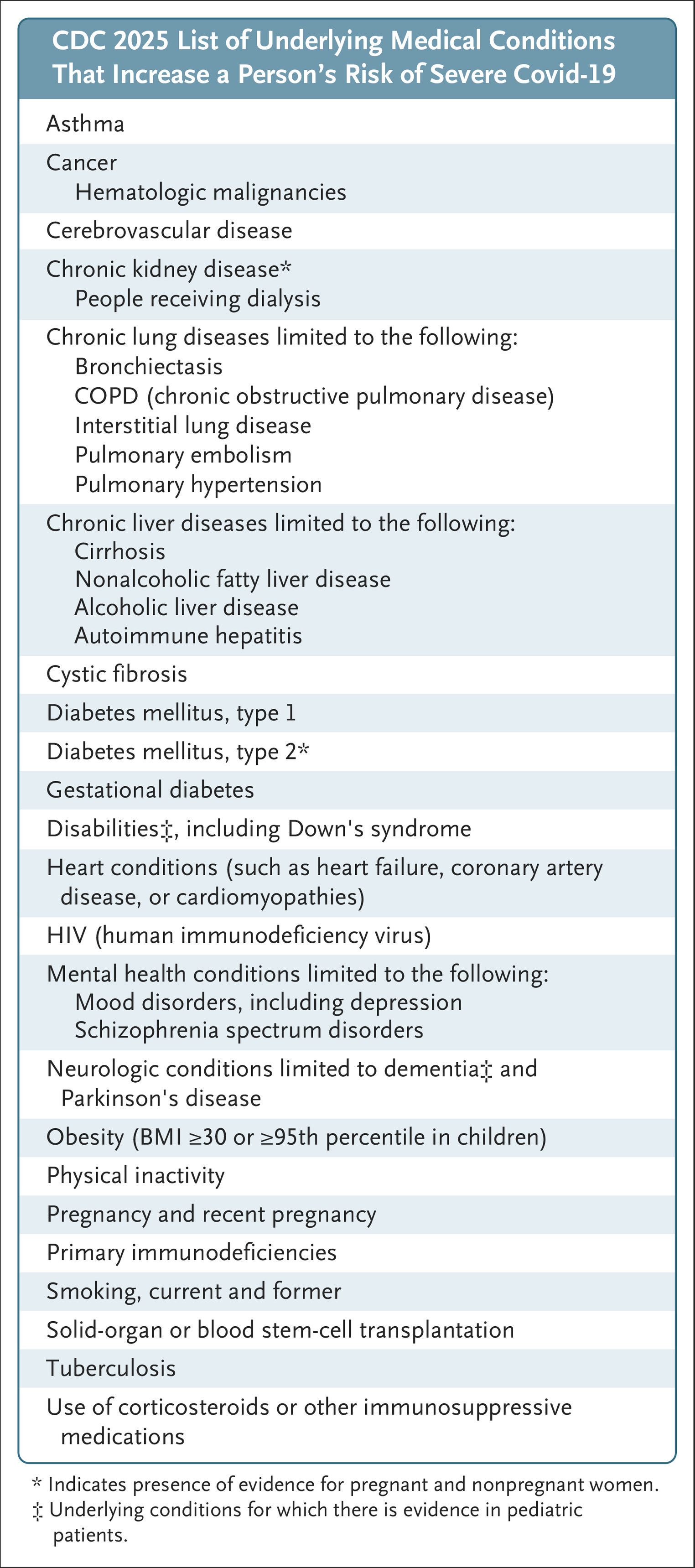
Know your options. The vaccine is not limited solely to those over 65; you may qualify for accessing vaccination if you have another health issue. Listed here, many people with long COVID meet at least one of the criteria. If you want to continue vaccination, it’s important to know your options.
A Moral Hierarchy of Who Deserves Help
Layered on top of these systemic failures is a dangerous cultural narrative about who deserves compassion. Government leaders like Mike Johnson argue that only the “deserving” poor - typically envisioned as the elderly, children, or struggling mothers - should have access to services like Medicaid or food stamps. Everyone else, particularly an able-bodied man, is expected to “man up,” find a job, and stop being a burden.
It’s as though illness itself is un-masculine, a moral failing that signals laziness or weakness. But disease does not discriminate. COVID-19, diabetes, depression, and cancer are not punishments for bad behavior. They are part of the human condition. The idea that only certain people are allowed to struggle is both dehumanizing and dangerous. We are all at risk. We all deserve protection.
A lifestyle that includes a wholesome diet, exercise, clean air, laughter, and community is one everyone deserves access to. These factors improve health and reduce the chances of disease, although we must also remember they do not prevent the possibility of disease. Unfortunately, this is a lifestyle many Americans do not follow, and when there is a pattern at scale like this, it is likely because of a systemic issue discouraging or disincentivizing it. Lifestyle “choices” of affordable food, clean air, and quality public education are not moral choices, they are the outcomes of government structure.
Vaccines, Medicaid, Medicare, mask access - these are not “handouts” for the morally weak. They are essential infrastructure built to ensure that everyone has a fighting chance when they need help most. Investing in these systems helps everyone, not just the most vulnerable.
Conclusion: DARVO Isn’t Just a Buzzword. It’s a Political Strategy
DARVO - Denial, Attack, Reverse Victim and Offender - isn’t just a pattern of abusive behavior, it’s increasingly a political tool. It allows those in power to escape responsibility by blaming the very people harmed by their policies. And it's being deployed at the highest levels of government to undermine the American public’s health, dignity, and agency.
So what can we do?
We stop accepting the blame. We reject the shame. And we turn toward one another.
It’s more important than ever to lean on trusted sources and supportive communities. The system may be shifting around us, but we are not powerless. When we rely on people who have our best interests at heart, whether it’s medical professionals, advocates, or peers who’ve walked this road before, we get smarter. We get stronger. We learn how to navigate around the barriers and still access what we need.
I have learned and continue to learn from others, and I am committed to remaining a support to you, as well.
Subscribe. Stay connected. Share what you learn. Together, we can see through these DARVO tactics, and perhaps build something better.