

Dizzy when you stand? It could be blood pressure—or your inner ear
Orthostatic intolerance and vestibular dysfunction can cause similar symptoms, but they are not the same problem—and don't have the same treatment.

I wasn’t sure what was happening, I just knew I couldn’t stand up
On my worst days with long COVID, I had to crawl to get from one place to another. There were two reasons.
First, like a lot of people after a COVID-infection I had developed POTS, a disruption of the autonomic nervous system (ANS). Among other things, the ANS controls blood pressure. Because it was disrupted, when I moved from lying down to standing, my blood vessels didn’t respond properly. My blood pressure dropped, my heart raced, and I felt like I would pass out, a sensation called presyncope. Presyncope was an alarm telling me to get horizontal and re-establish blood pressure.
POTS was fairly easy to diagnose, but there was another reason I was dizzy, and it took much longer to identify: my vestibular system was damaged.
The vestibular system is another branch of the nervous system that keeps us upright. By connecting the inner ear, brain, eyes, and muscles, it helps the body understand where it is in space. When it’s not working well, the vestibular system can cause dizziness—vertigo, to be precise—and many other symptoms: tinnitus, migraines, cognitive strain, visual overwhelm, and fatigue.
This is where things get tricky. Dysautonomia and vestibular dysfunction can look similar from the outside, and many patients—especially those with long COVID or chronic illness—may have features of both. If we assume all dizziness is from POTS or blood pressure, we may miss the vestibular system and miss out on treatment.
That’s important to recognize because, while vestibular damage is not always reversible, it is often treatable. The right evaluation and rehabilitation can significantly improve quality of life—but it’s got to be diagnosed first.
From my perch in the long COVID space, I’m relieved to see post-COVID dysautonomia becoming more recognized. But I worry we are still overlooking—and therefore under-treating—the vestibular system. For some patients, it may be why progress stalls.
So today, let’s learn the basics of this complex and fascinating system.
In this post, you’ll learn:
how the autonomic and vestibular systems work
why both can cause dizziness
how to start telling the difference between blood-flow dizziness and vestibular dizziness
which medical professionals can help
what treatment often looks like
This post is free. Please consider a paid subscription to support my effort to bring long COVID resources to those who need it.
Learn more about dysautonomia in my February interview with a Stanford scientist.
Stellate Ganglion Block for Long COVID

I’ve been getting messages about stellate ganglion block (SGB) from long COVID patients for years, often from people who either swear by or curse it. If you’ve researched it yourself, you may have found the same split. Why does this intervention—an injection targeting the nervous system
Blood-flow dizziness vs vestibular dizziness
The crux of the problem is in one word: dizzy. Both dysautonomia and vestibular dysfunction can make us feel dizzy. Or light-headed. Or like the room is spinning….Is there a difference?
There is. But “dizzy” is too vague to tell us which system is involved—or if both are involved.
Orthostatic dizziness includes:
Light-headedness
Feeling faint
Exhaustion
Symptoms are often worse with:
Standing
Heat (including showers)
Meals
Prolonged standing
Symptoms may improve when lying down.
Vestibular dizziness includes:
Vertigo: the room feels like it’s spinning
Rocking or swaying: you feel like you’re on a boat
Motion sensitivity/ nausea
Visual overwhelm
Feeling disoriented when moving through space
Unlike most autonomic causes of dizziness, vestibular symptoms can be triggered by:
Head movement: up, down, side to side
Rolling over in bed
Walking
Driving
Screens
Crowds
Diagnosis is not straightforward
If dizziness is mainly triggered by being upright, think about blood flow and the autonomic nervous system. If dizziness is triggered by head movement, tracking visual stimuli, think about the vestibular system.
Sounds simple to differentiate, right?
Perhaps in a textbook, but rarely in real life, especially with long COVID. Symptoms and triggers can be subtle and difficult to distinguish, both by patients experiencing them and physicians investigating. Remember, a single patient can have both issues (I’ll raise my hand here), which makes the investigation even more complicated.
Meet the vestibular system
The vestibular system is part of the body’s balance and orientation network. It begins in the inner ear, where motion-sensing structures called crystals, or otoconia, detect head movement and gravity.
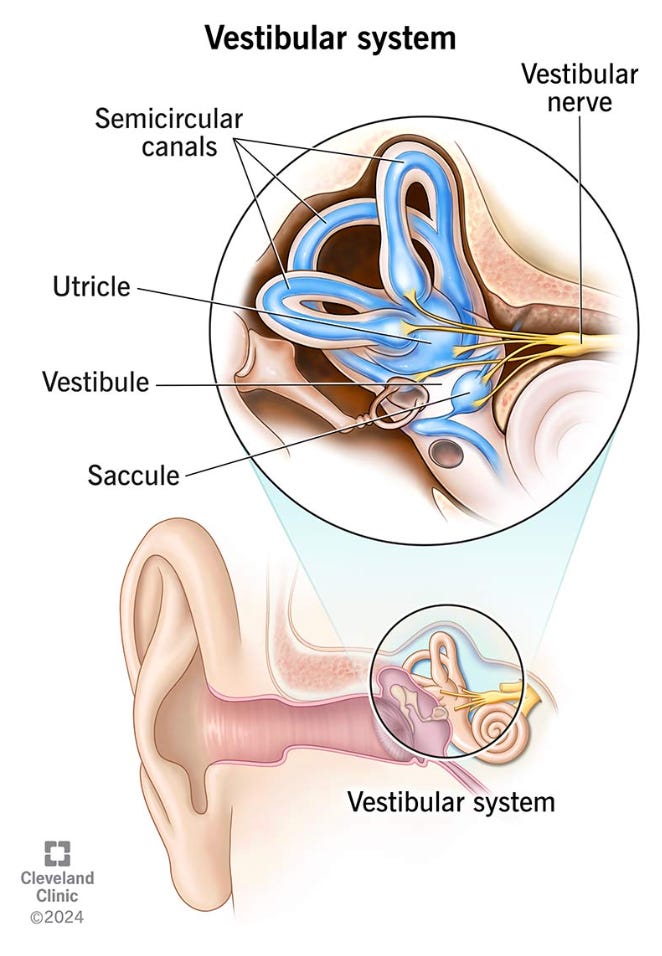
Signals travel from the ear through the vestibular nerve to the brainstem and cerebellum.
The brain then combines vestibular input with:
Vision
Muscle and joint position signals
Balance feedback from the body
The vestibular system helps the brain answer:
Which way is up?
Is my head turning?
Am I moving, or is the room moving?
How do I keep my eyes steady while my head moves?
How do I stay balanced while walking?
When your vestibular system is disrupted at any point along these pathways, the brain has a harder time locating your body in space. The world can feel unstable, even when nothing around you is moving.
What vestibular changes can feel like
When the vestibular system is disturbed, we have a harder time integrating information from the other organs in the network. This can happen after trauma, infection, and/or aging. Whatever the trigger, the vestibular system may explain why we get confused—and exhausted—with tasks that involve tracking (vision and head movement), multiple sounds (ears), and movement (walking).
Grocery Store Syndrome
After a COVID infection, many people report they have a hard time with tasks that used to be easy. Grocery shopping is a common example. It used to be so easy, why would it be hard now?
Let’s think about what a trip to the grocery store entails:
Lights
Sounds
People moving
Mapping locations of items
Keeping track of your grocery list
In formal terms, a trip to the store requires:
Memory
Attention
Executive function
Spatial navigation
Understanding the vestibular system, it’s easy to see how a grocery run could be an exhausting task. Remember, a vestibular problem does not always feel like dramatic room-spinning vertigo. It can feel subtler: disorientation, visual overload, unsteadiness that lasts a few moments, and nausea.
Fatigue and confusion commonly result after a trip like this, because it takes a lot of brain power to keep oriented, much less complete a multi-sensory task; your body is working really hard to support you.
An important reminder you to extend your body grace in this season. It’s not working perfectly, but it is working.
Why this matters in long COVID
COVID is known to impact the autonomic system and may impact the vestibular system more than we currently understand. It may link many of our seemingly unrelated symptoms, from dizziness to headache (specifically migraine), fatigue, tinnitus, and cognitive issues otherwise labeled “brain fog.”
How to evaluate vestibular dysfunction
Vestibular problems often require multi-specialty care.
Specialized clinicians
Neurology: the most helpful may specialize in migraine disorder
Otolaryngology: Ear, Nose and Throat physicians (ENT)
Neurotology: ENT physicians who specialize in the connections between the ear and brain
Neuroopthalmology: Eye physicians specialized in the connections between eye and brain
Audiology: a health professional specialized in testing and treating hearing disorders
Physical therapy specialized in vestibular or neurologic disorders
Specialized testing
A physical therapist trained in vestibular or neurologic rehabilitation can be hard to find, but well worth the search. Vestibular therapists are not doing the same work as general orthopedic physical therapy.
They may evaluate:
Eye movements
Balance
Gait
Head-motion tolerance
Visual dependence
How well the brain is compensating for altered vestibular input
Evaluation includes close attention to eye movements called videonystagmography, which uses an infrared camera to track how the eye responds to changes in your body’s position.
Treatments
Vestibular rehabilitation therapy
Vestibular rehabilitation therapy over several months is often helpful. This is an attempt to retrain the body’s balance system, and develop effective ways to compensate for brain pathways that have been lost.
This is not always an easy program, so expect to be challenged. Exercises include:
Gaze-stabilization
Balance training
Habituation exercises for motion sensitivity
Repositioning maneuvers for positional vertigo (the trained therapist may turn your head and body to re-align inner ear crystals)
Medications
Medications are aimed at symptom control, including:
Migraine treatment (several classes of medications and interventions fall in this category)
Short-term medication for nausea or severe acute vertigo, for example meclizine
A class of medications called SNRI (seratonin norepinephrine reuptake inhibitors) has been used off-label for vestibular migraines and vestibular dysfunction
Lifestyle modifications
Sleep, hydration and nutrition aimed at maintaining steady glucose levels can benefit both autonomic and vestibular issues. I recognize these easier said than done.
Specific modifications to help vestibular function:
Limit vision tracking
Smaller computer screens, 1 desk screen instead of 2
Limit phone scrolling: TikTok, YouTube shorts are especially triggering, as they require your eyes to move quickly and often
Limit triggering activities like driving, when possible
Limit sensory inputs by wearing:
Sunglasses
Headphones/ear plugs
Importance of differentiating cause
Dysautonomia and vestibular changes may present with similar symptoms, but treatment is quite different. Certainly, an improvement in one will help your overall function, but if both systems are involved, both require intervention.
Work with your healthcare team for a vestibular evaluation if you’re noticing dizziness with movement beyond standing, eye symptoms, migraine headaches, and/or nausea.
The vestibular system is only one potential cause, but if it is involved, evaluation and treatment may significantly improve your function, health and well-being.
What’s your experience?
Have you had a vestibular evaluation?
Do you have “grocery store syndrome”?
Is it hard to describe what your dizziness feels like?
Until next time,
Dr Zeest Khan
You describe whats been happening to me for five years now exactly. I've stopped driving and dread going shopping , wake up with terrible headaches and walk around like I'm on a boat in choppy waters. Thanks so much for this info , will share with my doctors.
Thank you Dr. I hope I can find someone here in Australia to check this and manage. So did you have rehab as well and can you share your experience?